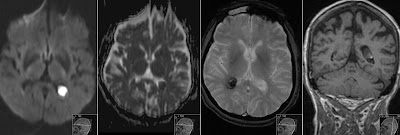
Transversal Diffusion Weighted sequence shows high signal in the left choroid plexus with corresponding low signal on ADC (restricted diffusion). Finding represents acute Hemorrhagic Choroid Plexus Cyst . It is also known as Choroid Plexus Xanthogranuloma . Gradient Echo sequence (third image) shows low signal in the right choroid plexus representing hemosiderine deposits after previous hemorrhage. Coronal T1 shows intermediate to high signal in the plexus cyst. Note also low signal in the right plexus on T2 (old hemorrhage) and high signal on FLAIR in the left plexus (acute hemorrhage). Choroid Plexus Cysts are very common normal finding. Those often show restricted diffusion. However in our case of patient with hypertension this finding is of interest to the clinicians as a requirement to more closely monitor patient's blood pressure. There were no signs of intraventricular hemorrhage.
Patient presented with expressive dysphasia . MRI shows acute infarct in Broca's Area in the left inferior frontal gyrus that is responsible for speech production. Note high signal on DWI, low on corresponding ADC as well as signal changes on T2 and coronal FLAIR.
10 years old boy from parents being cousins to each other presents with progressive rigidity and dystonia. Initial MR showing significant bilateral atrophy in caudate nuclei and putamina with high signal on FLAIR and T2 consistent with gliosis. Note striking symmetric atrophy of the putamina and caudate nuclei on T2 and IR. Huntington disease (HD) is also known as Huntington chorea. HD is an autosomal dominant chronic hereditary neurodegenerative disorder with complete penetrance [Osborn]. Aggregates of huntingtin protein accumulate in axonal terminals, which eventually leads to the death of medium spiny neurons. Autopsy shows generalized cerebral atrophy with an average of 30% reduction in brain weight. Both the cortex and hemispheric WM are affected. The most characteristic gross abnormality is volume loss with rarefaction of the caudate nucleus, putamen, and globus pallidus [Osborn]. Microscopically, HD features neuronal loss with huntingtin nuclear inclusi...