MELAS — Stroke-like Lesions

A patient with a known family history of MELAS (Mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes) presented with new neurological symptoms. On initial CT brain, there was a low-attenuation lesion in the right frontoparietal centrum semiovale that resembled a lacunar infarct.

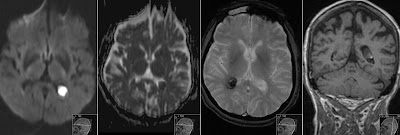
However, a follow-up MRI revealed:
• The lesion was hyperintense on DWI, but without corresponding ADC restriction — this indicates vasogenic edema rather than cytotoxic edema, which is not typical for an acute infarction.

• There was also evidence of old cortical volume loss in the same hemisphere, in the temporal lobe suggesting previous stroke-like episodes.

• Importantly, these lesions do not follow a specific vascular territory.
This pattern — recurrent, stroke-like lesions that spare strict vascular distributions and lack classic infarct diffusion restriction — is characteristic of MELAS. The underlying cause is mitochondrial dysfunction leading to metabolic failure and lactic acidosis, not thromboembolic vascular occlusion.
Key teaching point:
When you see cortical or subcortical lesions that look infarct-like but:
• Don’t respect vascular territories
• Have DWI hyperintensity without ADC restriction (vasogenic edema)
• Accompanied by cortical atrophy or other sequelae of prior episodes
…then consider MELAS, especially if there’s a supportive family history or clinical background.
Summary for students:
Not all DWI-bright lesions in the brain are infarctions. In MELAS, stroke-like episodes mimic strokes radiologically, but their mechanism is metabolic, so they don’t behave like true infarcts.