The Lasting Imprint of Poliovirus on the Spine and Musculature

Radiology Case Review: The Lasting Imprint of Poliovirus on the Spine and Musculature
While widespread vaccination efforts have made acute poliomyelitis a rare encounter in modern clinical practice, radiologists still frequently observe the chronic, lasting footprints of the virus in adult patients. Today, we are reviewing a fascinating and historically significant MRI case that beautifully illustrates the long-term sequelae of polio on both the central nervous system and the musculoskeletal system.
The poliovirus has a notorious affinity for the lower motor neurons, specifically targeting the anterior horn cells of the spinal cord. Decades after the initial infection, the resultant damage presents with a very characteristic set of imaging findings.
Let’s break down the key features visible in this patient’s scans.
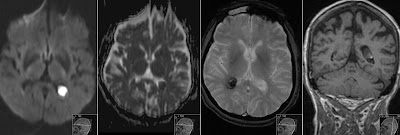
1. Symmetrical Anterior Signal Changes in the Spinal Cord
Looking at the axial T2-weighted images of the cervical spine, the pathophysiology of the virus is strikingly visible.
The Findings: Note the distinct, symmetrical hyperintense signal changes situated anteriorly within the spinal cord gray matter (highlighted by the blue arrows).
The Pathology: This is the classic "owl's eye" appearance (though varying in exact presentation), representing gliosis and the permanent loss of the anterior horn cells. Because the virus specifically attacks these motor neurons, the dorsal columns and sensory pathways are typically spared, which correlates perfectly with the purely motor deficits seen in these patients.
2. Pronounced Spinal Cord Atrophy
Moving to the sagittal T2-weighted images of the cervical and thoracic spine, the broader structural impact on the central nervous system becomes apparent.
The Findings: There is profound spinal cord atrophy. The cord is visibly thinned throughout the visualized segments.
The Pathology: This volume loss is a direct chronic consequence of the extensive motor neuron destruction. As the anterior horn cells undergo necrosis and clear out, the entire cord loses caliber over time, leaving a permanently atrophied appearance.

3. Profound Paraspinal Fatty Atrophy
The damage to the anterior horn cells does not just stay in the spine; the downstream effects on the musculoskeletal system are severe and characteristic. The axial slice of the lumbar spine provides a textbook example of chronic denervation.
The Findings: The arrows indicate the paraspinal musculature—specifically the erector spinae, multifidus, and the psoas muscles. Instead of healthy, dark muscle tissue, we see profound fatty replacement.
The Pathology: The high signal intensity represents severe fatty atrophy. This is not merely age-related degeneration or standard disuse atrophy; this is the end-stage result of chronic, irreversible denervation. When the lower motor neurons in the spine die, the muscle fibers they supply lose their trophic input, eventually shrinking and being entirely replaced by adipose tissue.
Summary Pearls for the Reading Room
When evaluating an adult spine with profound, symmetric muscle atrophy, always keep post-polio syndrome in your differential. Look closely at the spinal cord for:
Volume loss: Chronic spinal cord atrophy.
Signal abnormality: Symmetrical T2 hyperintensities in the anterior horns.
Downstream effects: Severe fatty replacement of the innervated musculature.
These images serve as a powerful reminder of the devastating anatomical impact of the poliovirus and the importance of correlating neuroimaging with musculoskeletal findings.

Watch Video on my YouTube channel Radiant Pixels
A Broader Look: Distinctive Signal Patterns in Spinal Cord Pathology
The classic "owl's eye" appearance of polio is just one example of how different diseases leave highly specific, geographic signatures on axial MRI slices of the spinal cord. Because the functional anatomy of the cord is so highly compartmentalized, the specific location of a lesion tells us a great deal about its underlying etiology.
I want to use this opportunity to present a quick review of the most characteristic cross-sectional signal patterns we encounter in spinal cord imaging:
Acute Transverse Myelitis (ATM), Neuromyelitis Optica (NMO), & ADEM: These inflammatory conditions typically present with central, expansile lesions. The signal abnormality is often broad, symmetrically involving both the central gray matter and the surrounding white matter tracts, frequently occupying more than two-thirds of the cross-sectional area of the cord.
Multiple Sclerosis (MS): In contrast to transverse myelitis, MS plaques are usually small, distinctly asymmetrical, and peripherally located. These demyelinating lesions have a strong predilection for the lateral and dorsal white matter columns and rarely involve the central gray matter.
Vitamin B12 Deficiency (Subacute Combined Degeneration): This metabolic condition presents with a highly specific, bilaterally symmetrical hyperintense signal confined to the dorsal columns. On axial imaging, this creates the classic "inverted V" sign. In severe cases, the lateral corticospinal tracts may also show symmetrical involvement.
Viral Myelitis (e.g., Polio): As demonstrated in today’s primary case, the poliovirus and similar enteroviruses selectively attack the lower motor neurons. This results in symmetrical, sharply defined bilateral signal alterations isolated strictly to the anterior horns of the gray matter.
Anterior Spinal Artery Infarction: Ischemia in this vascular territory affects the anterior two-thirds of the spinal cord. Imaging reveals a large area of bilateral anterior hyperintensity that involves the anterior horns and the anterior/lateral white matter tracts. Crucially, the posterior columns are completely spared, as they are supplied by the intact posterior spinal arteries.
Recognizing these specific spatial distributions is a fundamental skill in neuroradiology, allowing us to quickly differentiate between vascular, metabolic, inflammatory, and infectious etiologies.
*** > Author's Note: Images provided demonstrate classic chronic post-polio changes. Arrows indicate anterior horn signal changes (axial spine), and denervated fatty atrophy of the psoas and posterior paraspinal muscles (axial lumbar).