Dual Pathology in Epilepsy – Mesial Temporal Sclerosis, Frontal Contusions, and an Incidental Pontine Finding

When evaluating neuroimaging for epilepsy, finding a clear culprit is always a breakthrough. But what happens when the images reveal a more complex story—a "double whammy" of potential epileptogenic foci?
In the upcoming video on Radiant Pixels, we dive into a fascinating, longitudinal case of an epilepsy patient followed over a 12-year period (from age 30 to 42). This case beautifully illustrates classic mesial temporal sclerosis (MTS) while presenting an intriguing secondary structural pathology that poses a classic chicken-and-egg dilemma.
The Primary Suspect: Mesial Temporal Sclerosis (MTS)
The journey begins with a look back at the patient's scans from 12 years ago. On the coronal sequences—specifically using an inversion recovery sequence highly sensitive to anatomical structures—we see the definitive hallmarks of mesial temporal sclerosis:
Volume Loss: Clear, asymmetric atrophy of the left hippocampus.
Hyperintensity: Markedly increased signal intensity on the coronal FLAIR sequence.
Even though the patient’s current, recent scan is technically a bit more degraded in image quality, the structural reality remains identical: definitive left hippocampal gliosis and volume loss.

The Twist: Frontal Lobe Substance Loss
As we move more anteriorly, basally, and frontally, a second distinct pathology emerges. The axial and sagittal T2-weighted slices reveal focal substance loss and gliosis in the cortical and subcortical matter, specifically involving portions of the gyri recti.

This is highly characteristic of an old, traumatic brain contusion. This finding opens up a fascinating clinical discussion:
The Traumatic Seizure Mechanism: Did the patient experience a severe seizure with rapid head movement, resulting in a secondary contusion at the skull base?
A New Focus: Could these damaged frontal areas now serve as an independent, secondary focus for future seizure activity?

A Classic Bonus: Capillary Telangiectasia
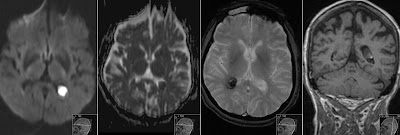
To wrap up the case, the older contrast-enhanced study offers an excellent teaching point. Centrally in the pons—a completely typical location—we find a diffusely defined, ~5 mm contrast-enhancing lesion.
There is no surrounding edema or mass effect.
On SWI (Susceptibility-Weighted Imaging), it shows a characteristic low signal.
This is a textbook, incidental capillary telangiectasia with no clinical consequences, but it serves as a wonderful reminder of what a benign brainstem mimic looks like in daily practice.
Flashback: This finding might look familiar to long-time readers of the blog. A while back, we analyzed a nearly identical presentation of a pontine capillary telangiectasia in another patient. You can review that previous case breakdown Capillary Telangiectasia to compare the signal characteristics on SWI.

Watch the Full Case Presentation
In the video, I walk through the timelines side-by-side, demonstrating how to optimize your evaluation of the hippocampi and navigate dual pathologies without missing incidental vascular findings.
Head over to Radiant Pixels to watch the full radiological breakdown, analyze the sequences yourself, and don't forget to like, subscribe, and share your thoughts on the case workflow in the comments section!