Gobbi CEC Syndrome (Celiac Disease, Epilepsy, and Cerebral Calcifications)

What do you do when a routine brain CT for non-specific headaches reveals striking, dense, bilateral calcifications, but the clinical exam is completely unremarkable?
In our latest teaching case on RP Radiology - Radiant Pixels, we break down a fascinating case of a 40-year-old patient whose neuroimaging keys open a door to a completely unexpected systemic diagnosis.
The Imaging Dilemma: Symmetrical but Atypical
When encountering prominent, symmetrical intracranial mineralization on a non-contrast CT, the classic reflex is to think of Fahr’s disease (primary familial brain calcification). However, this case reminds us why location is everything in neuroradiology. While Fahr's characteristically targets the deep gray matter, this patient's basal ganglia, thalami, and dentate nuclei were completely pristine. The dense calcifications were strictly restricted to the cortical and subcortical regions of the bilateral occipital lobes.
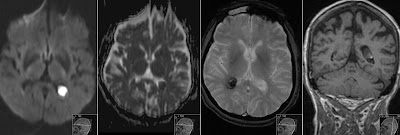
To investigate further, we performed an MRI, which revealed:
• Heavy blooming artifact on SWI, confirming the dense mineralization.
• Completely quiet parenchyma on FLAIR, with an absolute absence of surrounding edema or gliosis.
• No contrast enhancement or vascular malformations, effectively ruling out an atypical, bilateral presentation of Sturge-Weber syndrome.
Connecting the Dots: Gobbi (CEC) Syndrome
This precise neuroradiological signature—isolated, symmetrical occipital calcifications with spared basal ganglia and normal underlying parenchyma—points directly to a rare entity: Gobbi syndrome, also known as CEC syndrome.
CEC represents a distinct clinical triad:
1. Celiac disease
2. Epilepsy
3. Cerebral calcifications
Though traditionally diagnosed in pediatric patients presenting with occipital seizures, adult presentations can be completely asymptomatic or present with vague, non-specific symptoms like chronic headaches.
The Neurological Link to Celiac Disease
How does a gluten-induced autoimmune disorder cause intracranial calcifications? Celiac disease triggers an inappropriate T-cell-mediated response that damages the mucosal lining of the small intestine. This leads to chronic malabsorption of essential nutrients, particularly folate.
In the central nervous system, the combination of chronic folate deficiency and circulating immune complexes is thought to induce localized, low-grade endothelial inflammation. Within the posterior vascular bed, this microvascular injury ultimately results in the localized, dystrophic cortical and subcortical calcifications seen on our patient's CT.
As radiologists, recognizing this specific distribution allows us to guide the clinical team beyond neuroimaging. The vital next step for this patient isn't more scans—it's a simple celiac serology panel (anti-tTG IgA). Identifying silent celiac disease can prevent long-term systemic and malabsorptive complications.
Head over to the RP Radiology - Radiant Pixels YouTube channel to view the complete side-by-side CT and MRI walkthrough, analyze the imaging sequences, and add this high-yield differential to your diagnostic toolkit.