Intracranial Hypotension - Decoding the Intracranial Hemodynamic Paradox

Welcome back to the blog. In our latest case presentation on Radiant Pixels, we explore a fascinating neuroradiological riddle involving a 70-year-old patient. This case perfectly demonstrates how a familiar vascular pathology can completely mask a hidden, underlying mechanical issue.
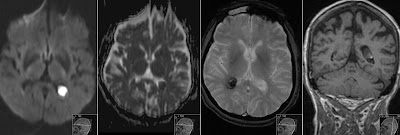
The Contradictory Imaging Findings
At first glance, the brain MRI presents a highly complex, multi-compartment constellation of findings:
Bilateral Chronic Subdural Hematomas (CSDHs): Measuring 3–4 mm both supra- and infratentorial, showing persistent enhancement one year after prior surgical evacuation via bilateral frontoparietal trepanation holes.
Chronic Dural Venous Sinus Thrombosis (CVST): A clear void of contrast enhancement centrally within the right sigmoid sinus and jugular foramen region, accompanied by a distended right jugular vein.
Diffuse Pachymeningeal Enhancement: Striking, smooth, generalized dural enhancement visible on post-gadolinium T1 sequences.
Pituitary Hyperemia: Upward bulging of the adenohypophysis, centrally touching the optic chiasm, with an internal cystic structure showing a chronic blood sediment level.
Brain Sagging: Lower positioning of the cerebellar tonsils showing slight ectopy, but without meeting the full criteria for a Chiari I malformation.
Normal Ventricles and Sulci: The ventricular system and cerebral sulci stubbornly maintain a completely normal size and configuration.
The Pathophysiological Logic: What is Primary?
In standard clinical practice, finding a chronic dural venous sinus thrombosis automatically leads our bias toward intracranial hypertension. However, evaluating this entire structural picture together reveals a brilliant pathophysiological twist: Spontaneous Intracranial Hypotension (SIH).
The timeline of this case is driven by a hidden CSF leak. According to the Monro-Kellie doctrine, because the skull is a rigid container, a primary drop in cerebrospinal fluid volume forces an obligatory, compensatory volume expansion elsewhere. The brain compensates by dilating its highly compliant venous networks.
This severe venous hypervolemia and localized venous congestion alter the intracranial environment in four distinct ways:
Dural Enhancement: The massive interstitial edema within the valveless dural capillaries causes diffuse pachymeningeal contrast enhancement.
Subdural Hematomas: The loss of CSF buoyancy causes the brain to sag downward, placing severe mechanical traction on the bridging veins, which leads to chronic, recurring bilateral subdural collections.
Pituitary Turgor: The rich, barrier-free vascular supply of the adenohypophysis undergoes intense hyperemia, causing the gland to swell and mimic an expanding or hemorrhagic cystic adenoma.
Secondary Thrombosis: The profound venous congestion slows blood flow within the large dural sinuses down to a crawl. This severe venous stasis—rather than a primary hypercoagulable state—is what ultimately precipitated the secondary chronic sinus thrombosis.
This explain why isolated surgical drainage of the subdural hematomas failed to resolve them after a year; as long as the underlying low-pressure CSF leak remains active, the venous congestion loop continues to pull fluid right back into the subdural space.
Watch the Full Imaging Breakdown
Want to see the side-by-side one-year follow-up comparisons, examine the pituitary sediment level, and review the exact slice locations for these findings?
Explore Previous Cases
If you enjoyed this hemodynamic deep dive, check out some of our previous related neuroradiology cases tracking complex intracranial pressure dynamics: